

Fit for Birth- essential exercises and helpful advice
Getting help
If you have any difficulty with the exercises in this booklet, or find that your symptoms are not improving, ask to be referred, or if available, refer yourself to a physiotherapist with experience in treating women with pelvic floor muscle problems.
To find your nearest specialist physiotherapist visit:
pogp.csp.org.uk
or contact:
POGP administration Fitwise Management Ltd. Blackburn House Redhouse Road Bathgate West Lothian EH47 7AQ
T: 01506 811077 E: info@fitwise.co.uk
Women with complex needs
If your ability to follow the advice in this booklet is affected by any health problem we suggest that you contact your local specialist women’s health physiotherapist, who will be able to assess you and offer specific alternatives, suitable for your needs.
Other booklets in this series available from pogp.csp.org.uk are Fit for Pregnancy, The Mitchell Method of Relaxation and Fit for the Future.
Glossary as the words occur in the booklet
pelvic floor muscles - the group of muscles spanning the base of your boney pelvis, held in place by ligaments which support the pelvic organs. Pelvic floor muscle exercises / Kegels will help keep these muscles strong
perineal/perineum - relating to the area between the anus and the vagina
contraction - a muscular tightening of the uterus. These are a sign of labour and become stronger and closer together
dilating/dilation - opening of the cervix
cervix - the lowest part of the uterus which opens up to allow childbirth. It connects the uterus and vagina. It can be felt at the top of the vagina; swabs of cervical cells are taken at your smear test
‘TENS’ - a Transcutaneous Electrical Nerve Stimulation machine is an electrotherapy treatment that can be used during labour as a form of pain relief.
isotonic drinks - a drink used to replace fluid and electrolytes lost during labour. Common examples are sports drinks
epidural - an injection into your lower back to numb the lower half of your body to stop you feeling any pain
placenta - an organ which joins you and your baby for exchange of nutrients. This has to be delivered after your baby
catheter - a tube put into your bladder to drain the urine (wee). Sometimes needed in labour
intra-abdominal pressure - an increase in the pressure in the tummy which causes strain downwards onto the pelvic floor muscles
uterus - the hollow organ in which the foetus/ baby develops in pregnancy (sometimes called the womb)
Fit for Birth
This booklet is designed to help you cope with your labour. It is recommended that you attend an antenatal class in your area if there is one available, in order to gain maximum information and advice.
It is highly recommended that you begin regular pelvic floor muscle exercises early in your pregnancy. This will help the muscles cope with the changes during the pregnancy such as the increasing load and the hormonal changes affecting your body throughout pregnancy and the post-natal period.
See other POGP booklets regarding further exercise advice and guidance.
Perineal Massage
Perineal massage from approximately 35 weeks pregnancy can reduce the likelihood of perineal trauma requiring stitches (in particular episiotomies) and women are less likely to report perineal pain at three months postnatally.
Using a natural oil such as coconut, Vitamin E or olive oil massage the perineum and vaginal opening (up to 4/5cms deep) with your index finger or thumbs; use circular or U-shaped movements firmly enough to cause a slightly uncomfortable stretch sensation. This can be done for 10 mins at least 2 times/week from 35 weeks of pregnancy.
Labour
First stage
During this stage, your contractions will be dilating (opening) your cervix (neck of womb) to allow your baby to be born; it is quite normal for this to feel uncomfortable or painful.
Some Pain Relief Options for this stage:
- Relaxation techniques such as the Mitchell Method, listening to music etc.
- Breathing techniques
- A warm bath or shower
- A TENS (transcutaneous electrical nerve stimulation) machine
- Comfortable positions (see below)
Early first stage
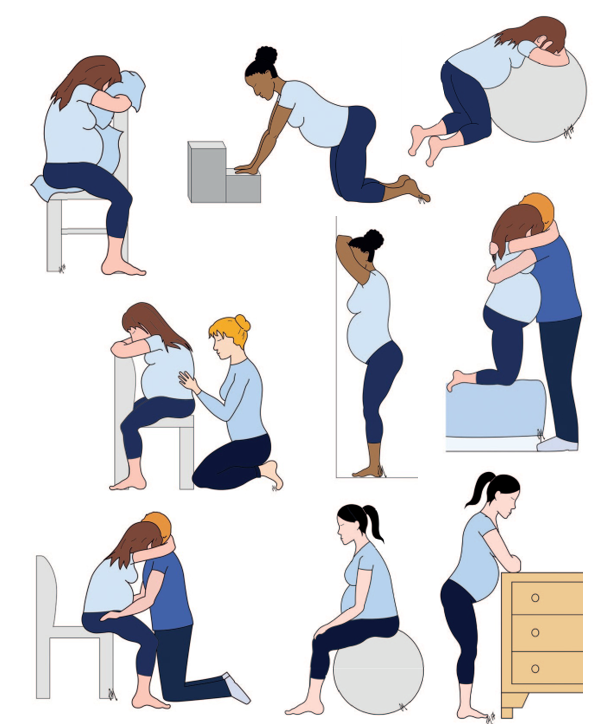
Being active helps with early labour and gravity helps labour to progress so it is important to be upright. You can lean forwards when resting. Activity such as walking, going up and down stairs, or sitting on your gym ball and moving your hips and pelvis can all help. The following positions may help with contractions or when you are resting. You can rock or circle your hips in any of these positions.
1 Sitting against a table relaxing forward or sitting facing backwards on a chair
2 Kneeling against a chair piled with pillows, or a beanbag or gym ball*, relaxing forward
* Please ensure the gym ball you are using is of ‘anti-burst/burst resistant’ quality and kite marked for safety
1 On all fours
2 Leaning against your partner
3 Standing, leaning forwards against the wall, or leaning your back against the wall with feet well forward
4 Sitting on a step, chair or gym ball, lean slightly forwards onto your lap
5 Leaning forward over a work surface or furniture
6 Sitting, using your partner for support
Your birthing partner can help by:
• encouraging you to relax and breathe calmly
• massaging your back
• suggesting a change of position, encouraging you to stay as upright and forward as possible
• cooling your face with a wet flannel
• offering sips of water
• giving you the support and encouragement you need
Fluid intake should be maintained throughout labour. You may find that isotonic drinks are more helpful than water in maintaining energy levels as well as hydration. A light diet should be maintained as guided by your midwife.
Some women may have the choice to labour in water (a bath or birthing pool) to help with the discomfort/pain.
As your labour progresses, your midwife will guide you about other forms of pain relief such as Entonox, Pethidine and epidurals. Where possible, you are encouraged to discuss all pain relief options with your midwife in advance.
If you choose to have an epidural, tell your midwife if, in pregnancy, you have had any discomfort or problems with your pelvis, back, hips or knees, so that she can help you into the best position for your delivery. See Pregnancy-related Pelvic Girdle Pain booklet (available for download at pogp.csp.org.uk).
Late first stage
Choose a comfortable position and try to relax to help you keep calm and conserve your energy. The contractions will now be much stronger and more painful. Think of them as ‘hills’ or ‘waves’ which you have to ride over on your journey towards the birth of your baby.
If your labour is long and difficult, you might want to accept further pain relief, in consultation with your midwife.

Managing Contractions
• Give a long sighing breath out when the contraction starts
• Your breathing may alter as the contraction builds. You may either hold your breath or breathe faster
• To help your breathing switch to ‘SOS’ (sighing out slowly) breathing. Your birth partner can encourage you with this
• Concentrate on ending each contraction with a long sighing breath out
• Try to relax your whole body completely before the start of the next contraction
As you progress from late first stage to second stage, your mood will alter; you may feel emotional, weepy, angry or tired. This is quite normal - your birth partner will be able to support and help you through this stage.
Second Stage
Your cervix has now dilated fully and you can actively help to push your baby out into the world. When you feel the normal desire to push, you should work with this feeling, adopting a position which is both practical and comfortable for you. Your midwife will guide you in pushing with your contractions and will usually be happy for you to adopt the position of your choice. ‘Listen’ to your body and be ready to change position if you feel the need. Sometimes the urge to push is felt before the cervix has become fully dilated; your midwife may ask you to pant or change position in order to relieve this.
The illustrations on this page show some positions for the second stage.

Breathe gently in and out as the contraction starts and when the urge overwhelms you, tuck your chin in and bear down towards your bottom, keeping your pelvic floor relaxed. Try not to hold your breath; instead,as you push, let your breath escape through yourlips - sometimes a groan or grunt helps! There will be several pushes in one contraction.
As your baby’s head is about to emerge, work with your midwife to control the speed of delivery; you willdo this by alternately pushing and panting or doing your ‘SOS’ breathing as she directs you.
NB If you have had any pelvic joint pain during pregnancy or in labour, tell your midwife who is delivering your baby. Pelvic pain may be experienced at the
front and/or back of the pelvis. Your specialist physiotherapist can recommend positions which may help in labour and delivery.
Sometimes labour does not go to plan and for various reasons you may be advised to change position or to have a caesarean section. The main goal is to make sure your baby’s health and your health is protected. Your midwife will guide you through your labour and support you in making choices.
Third Stage
During the third stage, the placenta (afterbirth) has to be delivered, and you may be asked to help by pushing.
After your baby is born... Pelvic floor muscle exercises
Your pelvic floor muscles may have been weakened by pregnancy and childbirth. To help strengthen them, you should perform pelvic floor exercises several times a day. Remember you can practise them in any position of comfort (eg while resting, or feeding your baby). They may also help to relieve any soreness. Whether or not you have stitches, remember to start gentle pelvic floor exercises as soon as possible after your baby is born. If you have a catheter, wait until this is removed and you have passed urine (had a wee) a couple of times before starting these exercises.
Improving your pelvic floor muscles
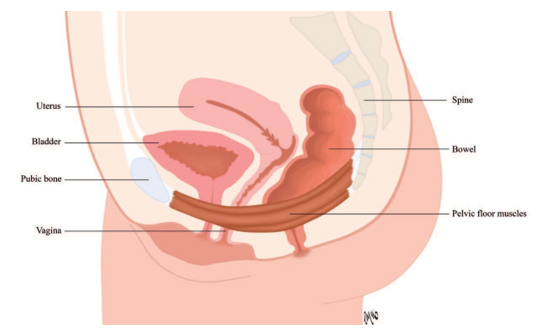
The pelvic floor muscles act like a hammock to support the pelvic organs. Pelvic floor muscle exercises will strengthen the muscles and retrain them to be effective in supporting the pelvic organs.
Pelvic floor muscle exercises should include long squeezes as well as short, quick squeezes. You should work the muscles until they tire and do the exercises regularly to help the muscles become stronger and more effective. Imagine that you are trying to stop yourself from passing wind at the same time as trying to stop passing urine. You should feel a squeeze and a lift inside. Do not hold your breath, do not clench your buttocks.
Long squeezes
• tighten your pelvic floor muscles, hold them tight, then release and let them fully relax. How long can you hold the squeeze?
• repeat the squeeze and hold until the pelvic floor muscles tire. How many times can you repeat the squeezes?
Short squeezes
• quickly tighten your pelvic floor muscles,then immediately let them go again. How many times can you do this quick squeeze before the muscles get tired?
• always let the muscles fully relax after each squeeze
Pelvic Floor Muscle Exercises
• aim to do 10 long squeezes, holding each for 10 seconds, relax the muscles for 10 seconds then do 10 short squeezes
• you may need to start with ‘little and often’ if you find that you can only hold the squeeze for a short time, or only do a few before the muscles tire
• you should do your pelvic floor muscle exercises at least 3 times each day. You may find it easier to start your programme when you are sitting or lying down
• build up your exercise routine gradually over the weeks and months. You should notice an improvement in 3 - 5 months and then keep practising your pelvic floor muscle exercises once a day to maintain the improvement
• eventually you can practise these exercises whilst doing activities such as walking and bending
The Knack
Draw up and tighten your pelvic floor muscles before activity that increases the intra-abdominal pressure (coughing/laughing/sneezing/bending), to help the pelvic floor muscles resist the downward movement of the pelvic organs, including the uterus.
It is important that you do your pelvic floor exercises correctly. Ask to be referred, or if available, refer yourself to a specialist physiotherapist as soon as possible after your delivery if:
• you are unable to perform a pelvic floor contraction, or are unsure if you are doing it correctly
• you leak wee or poo (urine or faeces), or cannot control wind
• your tummy muscles are doming upwards, gapping up the middle or are very weak
• you experience significant pelvic joint or back pain
• you experience discomfort during sexual intercourse once you have felt comfortable enough to resume sexual activity
Useful websites and further information
POGP booklets including Pregnancy-related Pelvic Girdle Pain for mothers-to-be and new mothers, The Mitchell Method of Simple Relaxation available for download at pogp.csp.org.uk
Patient information leaflets from the Royal College of Obstetricians and Gynaecologists at https://www.rcog.org.uk/en/patients/patient- leaflets/
NHS Choices patient information pages http://www.nhs.uk/ Search/?q=postnatal
Your local hospital’s website