

Baby Hip Health
The Parents' Guide
Introduction
At Steps, we understand how a lower limb condition can affect individuals, families, and communities. Our commitment is to helping people understand these conditions, offering reassurance and actively working for a better future, through our work with national health services and research projects. This booklet is for all parents. It explains why a baby’s hips are checked at birth, what the tests are and what happens if a problem is found. It also tells you how to keep your child’s hips healthy. It cannot tell you everything you need to know about what the future may hold, but we hope it will reassure you. It is also intended to show that practical help, specialist medical information, emotional support, and links to other sources of information are all available, if needed. This will help you to be more prepared for the road ahead and have information to hand so that you can ask informed questions about your child’s care, treatment, and prognosis.
Help When You Need It
Sometimes being able to contact someone who knows what you are going through can provide much needed encouragement. Our Family Contact Service can put you in touch with others who have shared a similar experience and can offer advice, support, and practical tips. You can also share your problems and solutions to everyday challenges on our closed Facebook Group for parents.
The group is a friendly and safe way of discussing online your worries with other parents, sharing tips, and finding emotional support. Remember, the STEPS Helpline team are here to offer information and support in total confidence and answer any questions or concerns you may have. This will help you to ask informed questions at hospital appointments or may help to reassure you along the way. No matter how big or small your concern, please telephone our Helpline on +44 (0) 1925 750271 or email info@steps-charity.org.uk for support and advice in total confidence.
How does a baby’s hip grow?
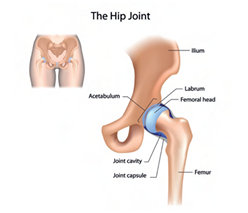
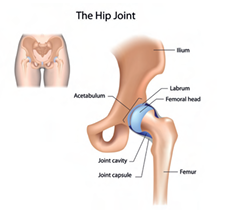
The hip joint is called a ball and socket joint. The top of the thigh bone is ball-shaped and fits into a socket on the side of the pelvis. This allows the leg to move both up and down and side to side. For the hip joint to grow normally the ball-shaped head of the thigh bone needs to be inside the cup-shaped socket. Very young babies’ hips are made of soft cartilage which changes into bone over the first few years. For the joint to grow properly the ball and socket have to be held firmly in the right place. It is held in place by ligaments, muscles, and a joint capsule.
Why are babies’ hips checked at birth?
It is estimated that approximately 1 in 10 newborn infants has hip instability. That means the hips can be wiggled in the socket because of loose ligaments. Most of these loose ligaments will tighten up naturally after birth.
Hip instability in babies is most frequently discovered at the time of the newborn physical examination by physicians, according to national screening pathways. The aim of the screening pathways is to identify all cases of hip instability so that observation and/or early appropriate treatment leads to normal hip development.
The challenge is to differentiate between a hip with instability that will spontaneously correct itself, from a hip with instability that may lead to symptoms and a severe diagnosis such as developmental dysplasia of the hip (DDH). We will cover what DDH is later in the publication.
Can the test pick up all hip problems?
The hip checks are not 100% accurate. The physical examination only detects hip instability at the time of the examination. Furthermore, physical examination of the hips requires skill and experience to perform. If the clinical examination is performed by untrained or inexperienced examiners, hip instability may not be detected, or conversely normal hips may be thought to have instability.
It is also important to understand that hip dysplasia is a developmental condition, therefore can develop at a later stage.
It is therefore important to be aware of the key signs of hip dysplasia in the first few years of life of your baby.
Potential symptoms may include:
- unequal leg lengths
- hip clunks or pops
- when changing a nappy one leg does not seem to move outwards as fully as the other or both legs seem restricted
- asymmetric buttock creases (though this is also seen in many normal babies)
- in older children a limp if one leg is affected or waddling walk if both hips are impacted.
DDH diagnoses can only be confirmed by either ultrasound or x-ray imaging.
When are the baby’s hips checked? Most national screening pathways recommend checking baby’s hips at birth and at 6-8 weeks.
The hips are tested as part of the national newborn physical examination which is usually carried out in hospital before you go home. Newborn checks typically cover eyes, testes, heart and hips.
The healthcare professional undertaking the examination should explain what it involves. The examination can be performed by a doctor, midwife, health visitor or a medical professional who has been trained to do the examination.
Do these checks cause my baby any discomfort?
The manipulation is very gentle and should not cause discomfort, but most babies will object to being examined however gently. It can help to calm your baby by giving a breast or bottle feed before the examination.
How are the hips checked at birth?
During the examination, the healthcare professional will note how your baby holds his or her legs at rest. They will check to see if the legs are the same length, lie in a similar position and whether the natural thigh creases at the groin are symmetrical.
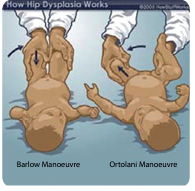
The baby’s hips are gently manipulated to see if they are safely in joint by tests known as the Ortolani and Barlow tests.
During the Barlow Manoeuvre, gentle downward pressure is applied to the leg to feel for the stability of the hip joint. The Barlow Manoeuvre is used to screen for a dislocatable hip (a dislocatable hip will be displayed out of the joint by this manoeuvre).
The Ortolani Manoeuvre is used to screen for a dislocated hip (a dislocated hip will be felt clunking into place).
In the Ortolani Manoeuvre, the baby is laid on his or her back and the hips are moved gently outwards. A distinctive ‘clunk’ (which is felt but not heard) suggests a possible abnormality and the joint may be classed as unstable. It may be caused by the head of the thigh bone moving in and out of the socket.
‘Clicky’ sounds are not usually important: a ‘clicky hip’ can be entirely normal.
When the test shows a potential problem, it is called a positive test, while a test that reveals no problem is called a negative test. The health professional will ask questions to find out if there are special risk factors that are associated with DDH. It is wise to discuss any family history of childhood hip problems now, if an opportunity has not arisen before.
What are the risk factors?
Hip dysplasia can happen to any baby but some factors, called ‘risk factors’, make the condition more likely.
Unfortunately, to date, there is no international consensus in deciding what constitutes a significant risk factor. National health systems will apply their own risk factors to determine if there is a need for an ultrasound.
The most common risks factors are:
- Breech presentation (bottom or feet first).
- Hip instability and/or physical signs suggesting a possible dislocated hip during a clinical examination.
- Positive family history such as mother, father, brother or sister, have had a hip problem treated as a child.
DDH is more common in first pregnancies and in baby girls. Babies with mild foot abnormalities or tightness in the neck are also more likely to be diagnosed with DDH.
My baby’s hip test is negative, but I have been told she/he still needs an ultrasound?
If your baby’s newborn physical examination is negative, but you have responded positively to one of the risk factors (i.e your baby was born breach or there is a family history of hip instability), you will be automatically recommended an ultrasound.
National pathways recommend an ultrasound study at six weeks of age for babies with DDH risk factors.
My baby’s hip test is positive, what happens next?
If during the newborn physical examination the healthcare professional identifies some form of hip instability, your baby will be referred for an ultrasound within 6 weeks.
Sometimes a baby’s hip stabilises on its own before the scan is due, but it is important the hips are checked to ensure that the hips are stable.
What is an ultrasound examination?
This is a harmless procedure very similar to ultrasound used in pregnancy.
Steps, in collaboration with the British Society of Children’s Orthopaedic Surgery (BSCOS) have produced a video to explain the ultrasound.
An ultrasound helps the doctors to obtain an accurate image of the hips to see if they are well-formed and safely in the right place. It can identify abnormalities of the shape of the ball and socket and see if the ball is unstable - whether it displaces out of the socket. These problems are not always felt when the hips are tested by hand. Sometimes, the ultrasound test may be normal when the physical examination suggested there might be a problem.

During the ultrasound examination, the hip is also examined for stability in the same manner as the Barlow test, but the ultrasound is used to see if the hip is unstable instead of relying solely on a practical examination by the doctor.
What happens after the scan?
At the end of the scan, the healthcare professional will discuss the results with you. If the ultrasound scan is normal, no further tests are required. It is, however, good practice to ensure that a baby’s hips are developing healthily by following a few tips as per the information on page 10.
If the first ultrasound scan shows that your baby’s hip is immature or has a borderline result, a repeat scan will be arranged for 4 weeks following the initial scan. Over this time, the hip may start to function normally and nothing else will be needed.
If an abnormality is seen on the second scan, you will be referred to a Children’s Orthopaedic doctor who will be able to start treatment if necessary.
What happens if they diagnose hip dysplasia in my baby? Why does hip dysplasia happen?
The exact cause or causes of hip dysplasia are not known and it is important to understand that it is not anyone’s fault. Even though as parents you may be concerned at discovering your baby has hip dysplasia, he or she will not be in pain. Hip dysplasia does not affect your baby’s development such as crawling or walking.
Although many people may think that Developmental Dysplasia of the Hip (DDH), is a rare condition, it is surprising to know that it is one of the most common hip conditions in children affecting 1-3% of all newborns.
It is widely recognised by health professionals and researchers that hip dysplasia develops around the time of birth. This is because the hip socket is shallower at birth which is a natural occurrence as the foetus grows in the womb and there is limited space for the baby to move. The shallow sockets may allow more flexibility for the baby to pass through the birth canal.
It is also important to know that expecting mothers make hormones that help ligaments relax during the birth. These relaxing hormones can stay in a baby’s bloodstream for a few weeks making it normal for babies’ hips to be ‘stretchier’ and looser shortly after birth. As girls usually have more loose ligaments than boys, they are more likely to have hip dysplasia. Statistically they are 4-5 times more likely to have a hip dysplasia diagnosis than boys.
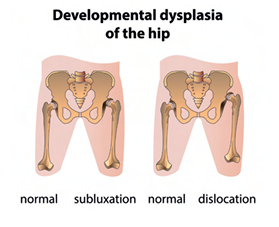
Loose ligaments mean that the hip is easier to be wiggled in the socket and, although in most of the cases ligaments tighten up naturally after birth, approximately 10% do not. If the ligaments around the hip joint are loose, the hip will subluxate. In medicine, a subluxation means that there is an incomplete or partial dislocation of a joint or organ. In hip dysplasia, this is when the ball is no longer centred in the socket.
What is Developmental Dysplasia of the Hip?
DDH encompasses a range of hip joint abnormalities, from mild instability to complete hip dislocations at birth. The hip joint is called a ball and socket joint. The top of the thigh bone is ball-shaped and fits into a socket on the side of the pelvis. This allows the leg to move both up and down and side to side. For the hip joint to grow normally the ball-shaped head of the thigh bone needs to be inside the cup-shaped socket. Very young babies’ hips are made of soft cartilage which changes into bone over the first few years. For the joint to grow properly the ball and socket have to be held firmly in the right place. It is held in place by ligaments, muscles and a joint capsule.
DDH means the ball and socket do not fit comfortably together: there are varying degrees of severity. If the ball (femoral head) is not held safely in place, the socket (acetabulum) may be more shallow than usual; this is called acetabular dysplasia. If the ball loses contact with the socket and stays outside the joint, it is called a dislocated hip. These are all forms of DDH. One or both hips may be affected.
What is the treatment for DDH?
This varies with the severity of the problem and the age of the child. Most babies are treated in some form of a splint, such as a Pavlik Harness, which keeps the hips flexed and abducted, so the legs are held splayed apart in the best position to encourage normal growth. The splints can be made from webbing, plastic, or plaster of Paris.
A few children’s hips do not respond to early treatment, and some are not detected until they are older. The approach to treatment for this group is different and a number of treatment options are available. These may include admission to hospital for special x-rays and a short period of traction, a small operation in the groin area under a general anaesthetic or a more extensive operation to put the ball and socket in place. After these more complex procedures it is normal to put the child in a plaster of Paris/fibre glass cast known as a hip spica - a full body cast enclosing one or both legs. Children who need to have their hips put back into place after infancy need to be monitored until they are fully grown.
Hip Health Guide
How do I look after my baby’s hip?
It is normal for a babies’ hips to be ‘stretchier’ and looser shortly after birth. Babies’ hips are always flexed so their thighs lie against their stomachs. They should be allowed to kick them straight on their own and not be stretched out. It is important to leave the hips free to move and not tightly strapped down with the legs straight out and pressed together. Let your baby hold his or her hips bent up as they were in the womb and allow room for the legs to move freely.
During the first six months of life, when the baby’s hips are growing rapidly, it is important to avoid activities or baby products that may affect hip positioning or hip motor development.
Should I swaddle my baby?
Swaddling infants with the hips and knees in an extended position increases the risk of hip dysplasia and dislocation. It is therefore important to use hip-healthy swaddling techniques to reduce this risk.
In order for swaddling to allow healthy hip development, the baby’s legs should be able to bend up and out at the hips. This position allows for natural development of the hip joints. The baby’s legs should not be tightly wrapped and pressed together.
Many parents prefer a ‘sleeping bag’ specifically designed for swaddling, instead of using a simple cloth or blanket. When purchasing a commercial product, you will need to ensure that it allows plenty of room for healthy hip positioning. It is vital that the product allows the hips to spread apart and bend up. Sudden straightening of the legs to a standing position can loosen the joints and damage the soft cartilage of the socket.
Can I carry my baby in a sling/carrier?
Any equipment that restrains a baby’s legs in an unhealthy position should be considered a potential risk for abnormal hip development. When choosing a product, it is important to assess the size of the baby, the length of time the baby will be placed in it and how the hips are impacted. The longer a baby is placed in a carrier that constraints the hips, the higher the chances are that the hips are impacted.
As such, if a sling is the preferred method to carry a baby around, it is important to chose one that promotes a healthy hip position during transport as per the picture below.
A properly fitting, wide-based carrier that promotes the M-shape, also known as the ‘spread squat’ or the ‘jockey position’, are common options. The M-shape is where the baby has their thighs spread around the mother or father’s torso. The baby also has the hips bent so the knees are slightly higher than their buttocks, or at buttock level with the thighs supported.
A good carrier should ensure that the thighs are securely supported all the way to the knees, which are held above the bottom. The hip joints are in the optimal position, and there is no weight at all dragging down on the joint.
In this picture we can see a mother carrying a baby with the thighs spread around the torso and the hips bent so the knees are slightly higher than the buttocks with the thighs supported. Parents are advised to research the general safety and risks of any device they wish to use. When in doubt, we recommend involving your primary health-care provider in any further decision-making that may be medically relevant.
For practical advice and Q&A with health professionals on DDH and the Pavlik Harness please visit our YouTube channel.
